In his presentation, neurosurgeon Dr. Galal Elsayed shows how spatial computing addresses this limitation. When surgeons understand patient anatomy in three dimensions before entering the operating field, intraoperative navigation becomes more predictable. Immersive preoperative planning combined with endoscopic visualization creates a continuous spatial workflow linking preparation and execution.
Preoperative spatial understanding
CT and MRI are usually reviewed on flat screens, requiring surgeons to mentally reconstruct 3D relationships from 2D slices. In MISS, where only a small region is visible, this cognitive step is demanding.
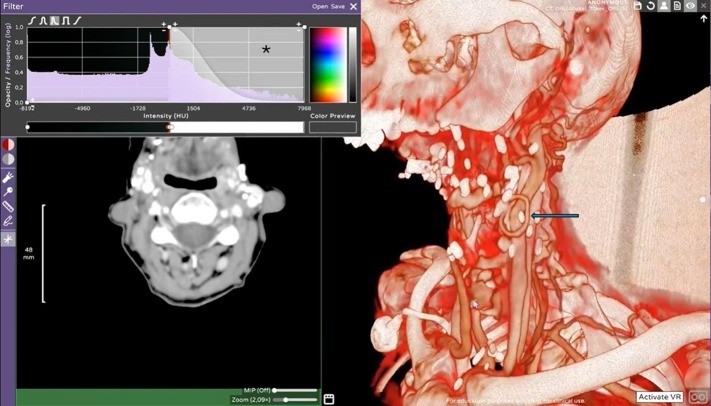
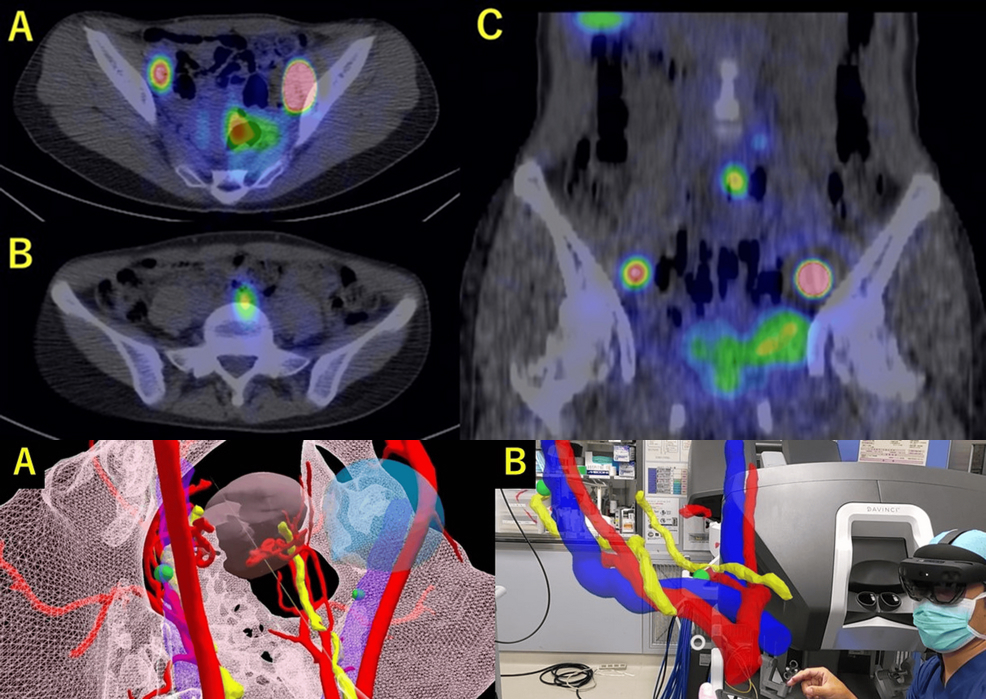
Immersive visualization converts patient-specific imaging into interactive 3D models explored in virtual reality. Surgeons can inspect vertebrae, discs, joints, and neural structures from any angle, simulate the surgical corridor, define the entry point, and anticipate variations such as deformity or migrated fragments. The result is a clear spatial plan: the access path, structures to avoid, and the extent of bone or ligament removal needed to reach the target safely.
Intraoperative endoscopic reality
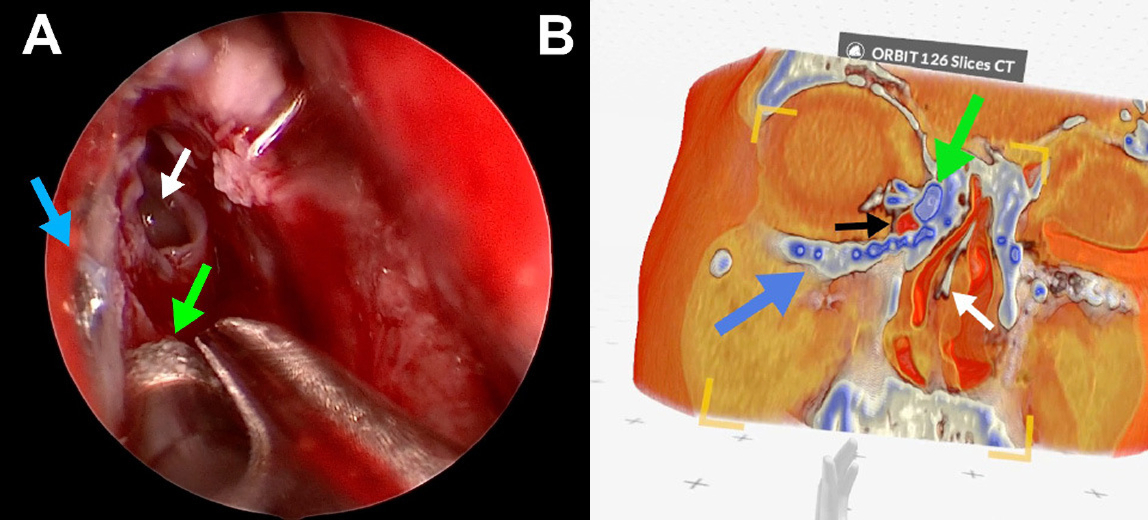
Endoscopy provides the real-time view through the minimal access channel, but it is inherently local. Only a small area is visible at once, and orientation depends on the surgeon’s internal spatial map.
With prior VR planning, this view gains context. Surgeons know what lies beyond the visible edges and how the current scene relates to the overall anatomy. The endoscopic image aligns with the previously explored 3D model, supporting confident navigation even in altered or degenerated spines.

Galal A. Elsayed, M.D is an Assistant Professor of Neurosurgery at Och Spine at NewYork-Presbyterian/Weill Cornell Medicine and serves as Director of Minimally Invasive Spine at Och Spine Queens. His clinical focus is on advanced techniques in spine surgery, with a special interest in minimally invasive and image-guided approaches.
Dr. Elsayed is also deeply involved in integrating extended reality (XR) and spatial computing into surgical planning and education, pioneering new ways to enhance precision and patient outcomes.
One continuous spatial workflow
The key innovation is integration. Preoperative VR exploration and intraoperative endoscopy form one spatial continuum: the surgeon first navigates the anatomy virtually, then reproduces this pathway in reality. Anticipated anatomy replaces intraoperative uncertainty, which is particularly valuable in complex cases.
Impact on training and reproducibility
MISS demands advanced spatial reasoning. Immersive planning allows surgeons in training to explore patient anatomy repeatedly before surgery, aligning mental models with operative views. This accelerates spatial understanding and shortens the learning curve.
Standardized 3D planning may also improve reproducibility. When corridors and targets are defined in a shared spatial environment, approaches become less dependent on individual interpretation of 2D images, supporting consistent outcomes and team communication.
Toward AI-supported minimally invasive workflows
AI-based segmentation can automatically identify vertebrae, discs, nerves, and pathology in CT and MRI, accelerating 3D model creation and highlighting relevant anatomy. This enables a streamlined workflow: automated reconstruction, immersive corridor planning, and intraoperative guidance aligned with the planned path.
From visualization to surgical workflow
Spatial computing is shifting from visualization to an operational component of surgery. In MISS, linking VR planning with endoscopic execution provides a continuous 3D understanding of anatomy, reducing uncertainty and improving precision.
Minimally invasive spine surgery will always involve narrow corridors. Spatial computing does not change the anatomy, but how surgeons perceive and navigate it. Integrating planning and execution in one spatial workflow points toward more predictable and teachable minimally invasive spine surgery.
Minimally invasive spine surgery is performed through extremely small corridors. Spatial orientation is limited. Learning curves are steep.
In his talk, neurosurgeon Dr. Galal Elsayed shows how spatial computing can change this.
By combining preoperative VR planning with intraoperative endoscopic visualization, surgeons gain a clear 3D understanding of anatomy before entering the operating field.
Patient-specific CT and MRI data are explored in virtual reality to define the optimal access path and anticipate anatomical variations. During surgery, endoscopy provides the real view through the minimal access channel. Together, planning and execution form one continuous spatial workflow.
This approach reduces uncertainty, supports navigation in complex or deformed spines, and shortens the learning curve for younger surgeons.
The perspective is clear: integrated VR planning, endoscopic surgery, and AI-supported workflows will make minimally invasive procedures more precise and reproducible.
Spatial computing is moving from visualization to surgical workflow.
For more information, contact info@medicalholodeck.com March 2026